The Garden Wall Problem: Why Your Insurance Type Determines Your AI-Ready Healthcare
In healthcare AI we focus on algorithms, models, accuracy. The quieter question: whose data can the AI actually see? The answer has less to do with the model and more to do with how you receive care. Your insurance type may determine whether your care is AI-ready at all.

When we talk about AI in healthcare, we often focus on the technology: the algorithms, the models, the accuracy metrics. But theres a more fundamental question were not asking: whose data can the AI actually see?
The answer depends less on the sophistication of the AI and more on something we rarely consider: the structure of how you receive care.
A Necessary Clarification
First, lets untangle the players, because much confusion comes from mixing roles:
- Insurance/payer decides coverage and reimbursement
- Provider delivers care and generates clinical dataHealth system governs workflows and records
- Patient experiences the fragmentation (or lack thereof)
AI readiness depends far more on care delivery and data governance than on the insurance product itself. But insurance models often correlate with care delivery structures, which is why the HMO vs PPO distinction matters.
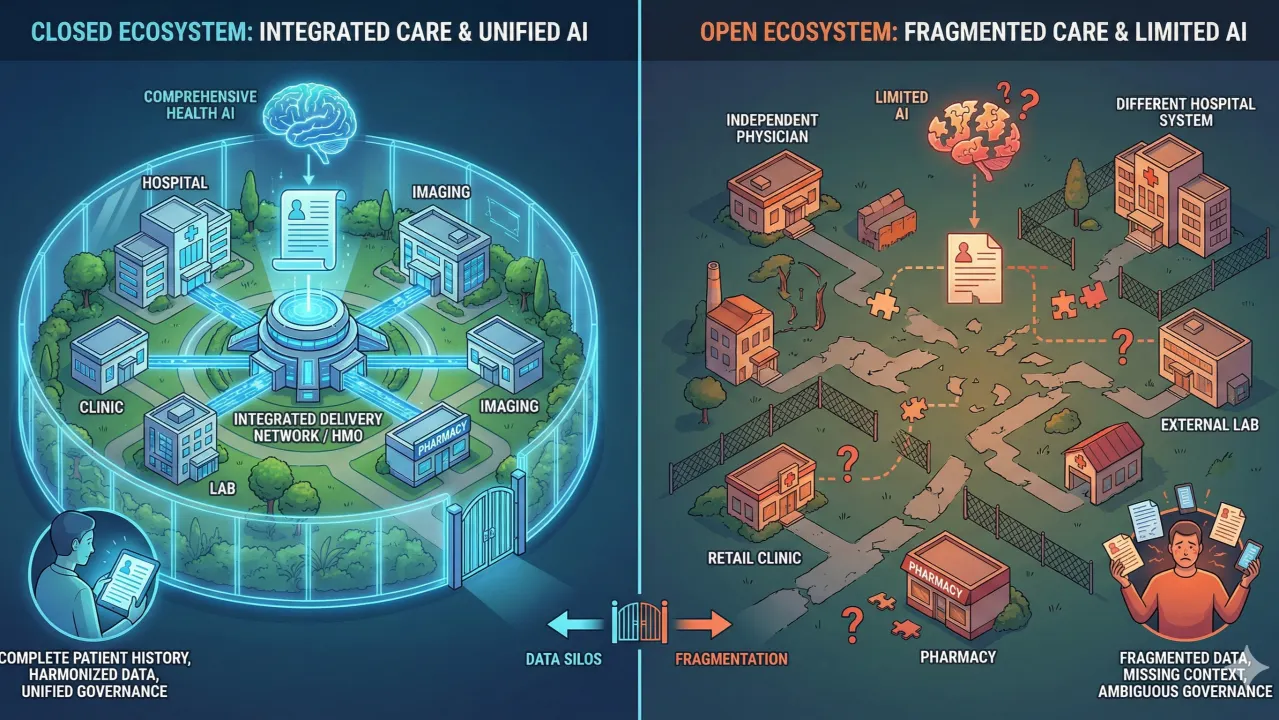
The Closed Garden Advantage: Integrated Care Models
HMOs and integrated delivery networks operate as relatively closed ecosystems. Patients receive most of their care from a defined set of providers, labs, imaging centers, pharmacies, and hospitals. Data sharing is imperfect, but it is at least designed to converge.
Consider Kaiser Permanente, the quintessential integrated system. A typical Kaiser member finds everything in one portal: visit notes, discharge letters, radiology images, lab results, occupational therapy records, prescriptions. Its not perfect, Kaiser Northern California, Southern California, Oregon, and Washington still run as independent organizations with separate medical record systems, but its remarkably unified compared to the alternative.
This closed garden approach creates ideal conditions for health AI. When most of your data lives in one ecosystem, AI tools can:
- Access a more complete patient history
- Train on harmonized, structured data
- Provide recommendations based on a fuller clinical pictureOperate under unified governance and safety protocols
Its similar to what we see in countries like Israel and the UAE, where near-unified health records create a foundation for reliable, comprehensive AI applications.
Even closed gardens still struggle with external data leakage, out-of-network care, and legacy systems, but they start from a position of accountability rather than diffusion.
New Closed Gardens Without Being HMOs
Not all closed gardens are HMOs.
One Medical, now part of Amazon, represents a newer, provider-led closed garden. While its not an insurer and doesnt operate as an HMO, it tightly controls care delivery, data capture, workflows, pharmacies, and patient experience within its network.
From an AI perspective, this matters more than the insurance label. Fewer systems, consistent workflows, and centralized governance make it far easier to build and trust AI tools, even if coverage and reimbursement still come from external payers.
The Fragmented Reality: PPO Plans and the Open Market
PPO plans represent the opposite extreme. Here, fragmentation is not a flaw. It is the design.
A typical PPO patients data is distributed across:
- Independent physicians
- Multiple hospital systems
- External labs and imaging centers
- Pharmacies
- Urgent care and retail clinics
Each provider holds a valid but partial view of the patient. No single entity is responsible for assembling the full longitudinal record. Integration is pushed downstream, often to the patient themselves and sometimes still using old fax machines.
For health AI, this fragmentation creates structural challenges:
- No true source of truth
- Missing context is the default
- Governance is ambiguous
- Validation becomes probabilistic rather than clinical
An AI tool might:
- Recommend a medication thats interact with something you're already taking (but its only recorded at the pharmacy)
- Miss a critical allergy documented at the hospital (but not shared with your PCP)
- Suggest a test you just had (but at a different lab system)
- Operate on 60% of your medical history and call it complete
Consumer Aggregation Is Not Clinical Integration
Platforms from Apple and OpenAI allow individuals to link records and aggregate data at the consumer level. This is valuable, but its not the same as clinical-grade integration - data is duplicated, units are not harmonized, the same drugs and sometime active conditions can appear under different names.
These approaches are:
- Voluntary
- Incomplete
- Dependent on patient action
- Limited by what providers expose
They help people understand their data, but they dont create the quorum of information clinicians rely on to act safely. Even when data can be connected, its often in incompatible formats, missing context, or riddled with gaps.
The AI Readiness Gap
The irony is stark: the patients who might benefit most from AI-powered care coordination, those navigating complex, fragmented PPO networks, are the least likely to have AI that actually works for them. Meanwhile, patients in closed garden systems get increasingly sophisticated AI tools built on more complete, governed datasets.
This isn't just a technical problem. Its a structural one. Were trying to build 21st-century AI on care delivery models that were never designed for data integration.
What This Means Going Forward
If were serious about health AI that works for everyone, not just those in integrated systems, we need to solve the fragmentation problem first. That means:
- True interoperability standards that actually work
- Patient-controlled health records that follow you
- Incentives for providers to share data, not hoard it
- AI architectures designed for incomplete, messy data
Or we accept a two-tiered future: sophisticated AI for the closed gardens, and limited tools for everyone else.
Health AI is not just a modeling problem. It is an architectural and organizational one.
The quality of your healthcare AI wont just depend on the algorithm. It will depend on whether your care delivery model came with walls or gates.
Dr. Yoram Friedman is a physician turned product manager with over 20 years of experience in enterprise software and digital transformation. He believes healthcare AI must rightfully earn its place through workflow, trust, and real-world outcomes.


